The tongue is a very dynamic structure. It is the only muscle (or group of muscles) that has a freely moveable end. Myofunctional therapists and others emphasize the importance of the tongue being able to rest on the palate during its resting state for proper craniofacial development. Tongue ties have been found to anchor the tongue to the floor of the mouth making it physically difficult for the tongue to rest against the roof of the mouth properly.
By naturally resting on the palate, a normally developed tongue widens and brings down the palate. Babies with tethered tongues are commonly born with high-vaulted, narrow palates. Besides making normal breastfeeding difficult, a high arch promotes mouth breathing along with a series of many other problems that I will not get into here.
The importance of resting tongue posture on the palate is emphasized for normal craniofacial development. What I want to describe in this article is a mechanism on how this widening and lowering of the palate takes place. As far as I know, I have not heard others describe it although I do not take credit for this idea.

The tongue on the palate itself is not a static structure. Physically taking up space on the palate does not solely promote widening and lowering. If that were the case one should expect that by placing the tongue on the palate, the arch would be raised because the tongue would then be putting an upward pressure on the palate.
But this is not what happens. Because the tongue does not act like a static structure on the palate. Even when the tongue is resting on the palate, it is going through a dynamic motion. It is this motion that I believe is what promotes the widening and lowering of the arch.
There are several motions that take place simultaneously. In reality they’re all part of the same motion and they are most pronounced with the breath. Let’s break them up for purposes of explanation:
Widening/narrowing:

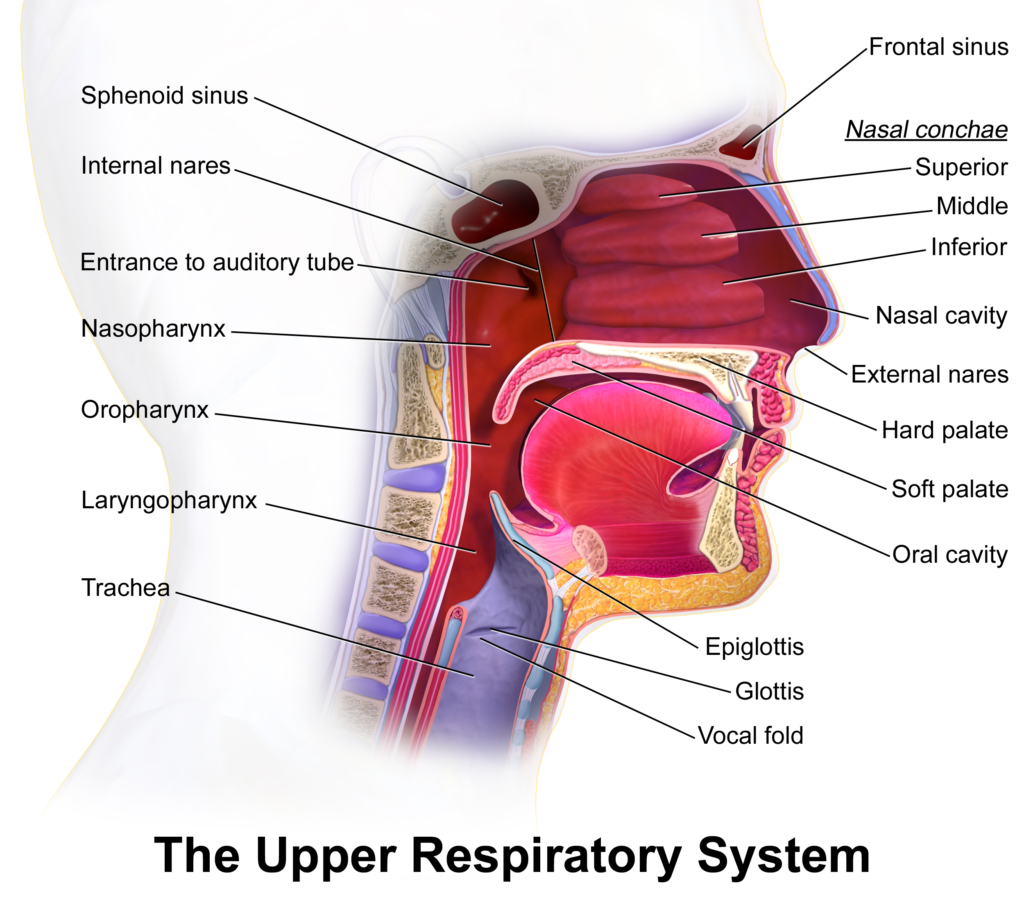
During the inhalation phase of a breath the front of the rib cage rises. As it does so, the trachea and hyoid in the neck rise upward slightly. During exhalation, the front of the rib cage lowers and the trachea and hyoid drop back down. The trachea acts like a slow moving piston. When the trachea lifts up, the tongue also lifts against the palate. The tongue is compressed or “squished” against the palate and so the tongue maintains its volume by changing its shape.
Part of this shape change is a widening of the tongue blade during inhalation and narrowing during exhalation. When it widens side to side it becomes shorter front to back. Furthermore, during this widening and narrowing of the tongue as it rises toward the palate and back down, there is a suction motion that happens. What this means is the tongue is dynamically widening the palate while at the same time through suction, pulling the palate down.
Forward/backward:
When the tongue rises against the palate, the tongue is driven forward. During exhalation, the tongue recedes backward and the trachea is drawn back down simultaneously. The trachea is not moving up and down on a purely vertical axis. The axis where motions is up and down like a piston is mostly vertical but also angled slightly towards the front of the mouth. As a result, the tongue also moves forward when they rise together.

Even though the tongue is widening and it is becoming shorter front to back (which would pull the tip back as the tip widens), the tongue is still moving forward and driving the palate forward. This motion allows the tongue to expand the palate in a forward direction while at the same time expanding the palate wider.
Expansion/recoil:
So similar to how the rib cage is going through expansion and recoil during inhalation and exhalation, the same is happening to the tongue. When the “piston” motion moves upward and the tongue is compressed up against the palate it moves outward and forward. Being suctioned to the palate when the piston motion moves downward, the tongue is pulls downward decompressing it from the palate and slightly pulling the palate downward with a negative pressure.
It is this constant dynamic motion of the tongue that helps the palate develop properly. Without the tongue on the palate, the tongue cannot do this and the end result is a high-arched, narrow palate.
Some may argue that without a developing baby breathing, this wouldn’t work in utero as a baby is developing. Osteopathic physicians for decades have described this motion throughout the body called the “primary respiratory mechanism.” This motion happens in all living beings all the time and is in addition to the breathing we all tend to think of. The primary respiratory mechanism is a inhalation/exhalation that is similar to the effects of the other respiration.
Therefore, even though a developing baby is not breathing oxygen directly, their tongue is still going through the same motions if the developing baby is able to properly rest their tongue on the palate. Even without breathing oxygen, the diaphragm does move in utero (which can be evidenced by hiccups) so the motion is still taking place.
With tongue ties, the degree to which the tongue is anchored will proportionately have an impact on how high and narrow the arch will be when the baby is born and if left unreleased, as the baby grows up to adulthood.
In conclusion it is known that the tongue and its resting tongue posture on the palate are important in craniofacial development. However, I always felt like the tongue being there itself was not sufficient in driving the expansion and lowering of the palate.
In this post, we have described a constant motion that one can feel (if they’re not too tongue tied) that I feel drives the normal craniofacial development. The tongue being unable to rest on the palate, will lessen or prevent this motion and the result is a narrow, high-arched palate.
I describe this motion and other concepts on this podcast here.
For those of you who want to experience this motion themselves, I have recorded a guided meditation to explore not just this motion in the tongue, but how it is connected to the rest of the body. Grab your copy by clicking on the picture below.


















Onohig Amoxiqio jrz.yorw.daniellopezdo.com.bce.di http://slkjfdf.net/
great information, enjoy and share it.https://social.msdn.microsoft.com/Profile/Contusion.Co
https://www.intensedebate.com/people/contusionco
https://www.openstreetmap.org/user/ContusionCo
https://letterboxd.com/contusionco/
https://thehub.io/startups/contusionco
https://contusionco.contently.com/
https://www.indiegogo.com/individuals/32984308
https://www.bark.com/en/us/company/contusionco/GpmRe/
https://forum.repetier.com/profile/contusionco
https://www.flickr.com/people/197891816@N02/
What’s up, all is going well here and ofcourse every one is sharing data, that’s in fact good, keep up writing.
hydrochlorothiazide 12.5mg
Appreciate the recommendation. Let me try it out.
promethazine generic
I think the admin of this web page is truly working hard
in support of his web page, as here every information is
quality based data.
cheap fluoxetine
Hello there, I believe your web site may be having internet browser compatibility problems.
Whenever I take a look at your blog in Safari, it looks fine however, when opening
in IE, it has some overlapping issues. I
merely wanted to give you a quick heads up! Besides that, wonderful website!
benadryl pink pills
I think that is among the such a lot significant information for me.
And i’m happy studying your article. However want to statement on few
normal things, The site taste is great, the articles is in reality nice : D.
Good task, cheers
buy lisinopril
https://independent.academia.edu/MilialarOfficial
https://crivva.com/members/milialar/
https://techplanet.today/member/Milialar
https://milialar.livejournal.com/
https://themediumblog.com/author/milialar/
https://sharefolks.com/Milialar
https://mtekcorp.mn.co/members/22247002